
Diagnosis
The diagnosis of AN has good reliability and validity and it is a relatively straightforward one. The major obstacle to diagnosis is if the patient does not want to willingly disclose their behaviors and symptoms.(1) Therefore, engagement in an empathic and supportive assessment interview is needed to help the individual reveal their symptoms and behaviours. Moreover, physical features of starvation and secondary amenorrhoea should alert physicians that AN may be the diagnosis. Another challenge occurs when the patient presents with conditions that mimic anorexia.(1)
1. Refer to table 3 or the DSM-IV-TR diagnostic criteria for AN.
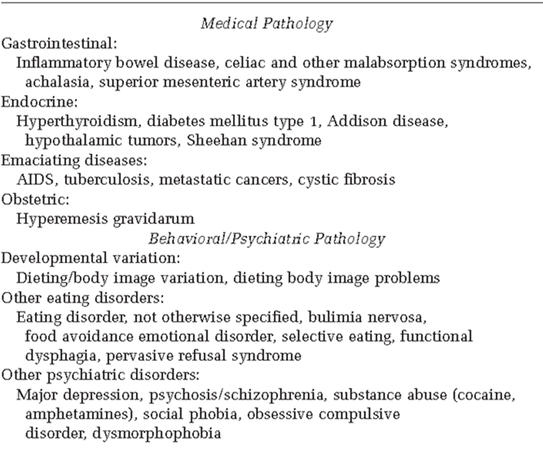
2. Rule out conditions that mimic anorexia (e.g. cause weight loss or amenorrhea). Refer to table 4 or a description of the differential diagnosis of anorexia.
Note: Depression, schizophrenia, and obsessive-compulsive disorder (OCD) can be a part of AN; therefore these disorders should be part of the differential diagnosis for AN7. Differences that are relatively specific for AN include a disturbed body image and a drive for thinness.(2)
1. Refer to table 3 or the DSM-IV-TR diagnostic criteria for AN.
2. Rule out conditions that mimic anorexia (e.g. cause weight loss or amenorrhea). Refer to table 4 or a description of the differential diagnosis of anorexia.
Note: Depression, schizophrenia, and obsessive-compulsive disorder (OCD) can be a part of AN; therefore these disorders should be part of the differential diagnosis for AN7. Differences that are relatively specific for AN include a disturbed body image and a drive for thinness.(2)
Table 3."DSM-IV-R Diagnostic Criteria for Anorexia Nervosa"(4)
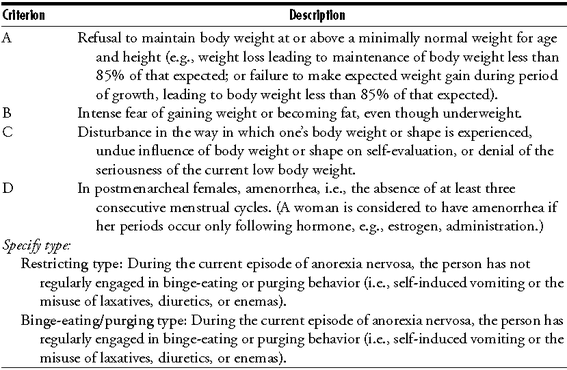
Table 4. Differential Diagnosis of Anorexia Nervosa (3)
References
1. Eating Disorders: Core Interventions in the Treatment of and Management of Anorexia Nervosa, Bulimia Nervosa and Related Eating Disorders. National Institute for Clinical Excellence, Clinical Guideline 9. http://www.nice.org.uk/CG009. pdated January 2004. Accessed June 1, 2013.
2. Talbert RL, DiPiro JT, Matzke GR, Posey LM, Wells BG, Yee GC. Chapter 64. Multiple Sclerosis. In: Pharmacotherapy: A Pathophysiologic Approach. 8th ed. New York: McGraw-Hill; 2011.http://www.accesspharmacy.com/content.aspx?aID=7984977. Accessed June 1, 013.
3. Silber TJ. Anorexia ervosa among children and adolescents.Adv Pediatr. 2005;52:49-76.
4. Treatment of patients with eating disorders,third edition. American Psychiatric Association. American Psychiatric ssociation. Am J Psychiatry. 2006;163(7 Suppl):4-54.
1. Eating Disorders: Core Interventions in the Treatment of and Management of Anorexia Nervosa, Bulimia Nervosa and Related Eating Disorders. National Institute for Clinical Excellence, Clinical Guideline 9. http://www.nice.org.uk/CG009. pdated January 2004. Accessed June 1, 2013.
2. Talbert RL, DiPiro JT, Matzke GR, Posey LM, Wells BG, Yee GC. Chapter 64. Multiple Sclerosis. In: Pharmacotherapy: A Pathophysiologic Approach. 8th ed. New York: McGraw-Hill; 2011.http://www.accesspharmacy.com/content.aspx?aID=7984977. Accessed June 1, 013.
3. Silber TJ. Anorexia ervosa among children and adolescents.Adv Pediatr. 2005;52:49-76.
4. Treatment of patients with eating disorders,third edition. American Psychiatric Association. American Psychiatric ssociation. Am J Psychiatry. 2006;163(7 Suppl):4-54.
