Complications
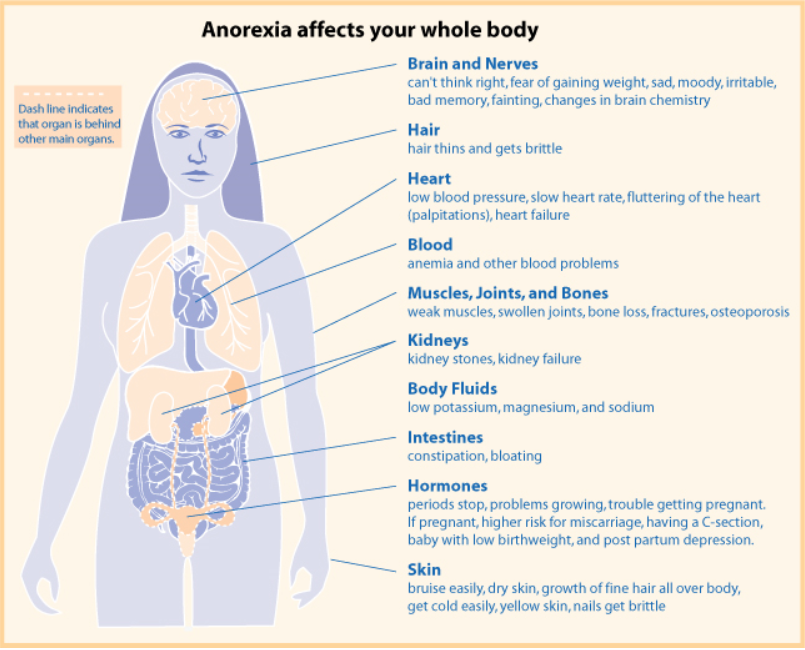
Weight loss and malnutrition cause the medical complications of AN. Starvation causes fat and protein catabolism, which leads to decrease in cellular volume and atrophy of the brain, heart, liver, kidneys, intestines, and muscles. As the
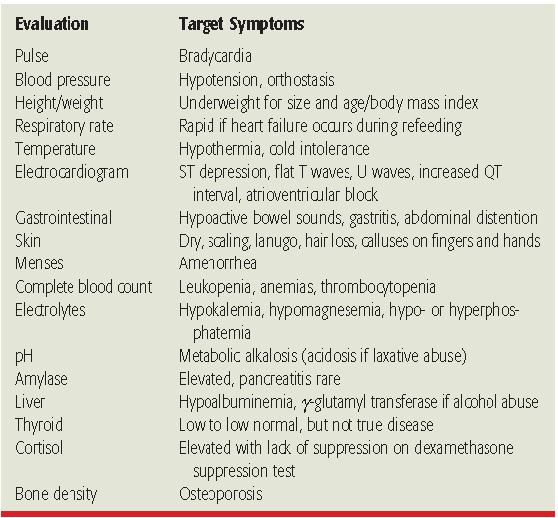
severity of illness increases more organ systems are adversely affected. To determine the severity of complications a thorough laboratory and physical evaluation is needed.(1) The laboratory and physical evaluation is described in table 6 For more specific details of the signs, symptoms and laboratory testing of each complication refer to table 6 of the American
Psychiatric Association (APA) guidelines.(2) Nutritional replenishment is part of the treatment for each complication. Upon weight gain many complications resolve.(1)
severity of illness increases more organ systems are adversely affected. To determine the severity of complications a thorough laboratory and physical evaluation is needed.(1) The laboratory and physical evaluation is described in table 6 For more specific details of the signs, symptoms and laboratory testing of each complication refer to table 6 of the American
Psychiatric Association (APA) guidelines.(2) Nutritional replenishment is part of the treatment for each complication. Upon weight gain many complications resolve.(1)
Cardiovascular
Structural Canges
Structural changes include reduced cardiac chamber volumes, decreased cardiac mass, atrophy of cardiac muscle, and mitral valve prolapse. These changes lead to subjective fatigue, decreased cardiac output, a decreased blood pressure response to exercise and reduced exercise capacity. The weakened heart muscle normally improves and heart size normalizes with weight gain and clinical recovery.(1)
Chest pain or palpitations may occur due to mitral valve prolapse. Additionally, HDL may increase because of weight loss and excessive exercise. There may also be insignificant elevations in LDL, however obstructive coronary disease was not revealed in autopsy studies. Furthermore, pericardial effusion is another complication that has been reported in adolescents.(1)
Functional Changes
Functional changes include hypotension, QT dispersion, diminished heart rate variability and bradycardia. In some patients QT prolongation may occur however, it is not clear whether it is a direct result of AN. (1) The ECG is often normal with the exception of bradycardia. QT dispersion may be caused by direct injury to the myocardium during starvation and is a marker for increased arrhythmic risk. Reduced heart rate variability may be associated with an increased incidence of death in AN. Furthermore, orthostatic hypotension may occur and depending on the severity may require hospitalization.(1)
Bradycardia
In a study of anorexic women, 41% were found to have bradycardia. Increased parasympathetic activity appears to be the cause of bradycardia.(1) Hospitalization is suggested by the APA guidelines if heart rate is less than 0 beats/minute. This complication normally resolves once weight is restored.(2)
Endocrine
Hypothalamus and pituitary
Starvation results in reduced secretion of gonadotropin releasing hormone, which leads to reduced levels of luteinizing hormone and follicle stimulating hormone. (1,3) Ultimately this causes amenorrhea and prevents ovulation. Moreover, there is evidence of elevated blood levels of cortisol secondary to an "increased activation of the hypothalamic-pituitary-adrenal
axis". Decreased blood levels of testosterone results in diminished production of androgens. Additionally, libido and a diminished anabolic state occur secondary to reduced testosterone. Bone formation is impeded because of decreased production of insulin-like growth factor. Furthermore, hypothermia was found in 22% of patients in a study.(1)
Osteoporosis
Osteoporosis is a potential long-term complication.(3) Amenorrhea for 6 months and a BMI of 15 kg/m2 can result in a decreased bone mineral density, which correlates with the degree of osteoporosis. The osteoporosis in postmenopausal women differs from the osteoporosis in patients with AN. For example, there are normal serum levels of vitamin D, parathyroid hormone and calcium in AN patients with osteoporosis. Resumption of menstrual function and
weight gain is the best treatment.(1)
Thyroid
Euthyroid hypothyroxinemia may develop. A normal serum level of TSH, decreased or normal serum levels of T3 and T4, and increased serum level of reverse T3 characterizes this complication. Thyroid hormone replacement is not indicated because it is not beneficial and it may be harmful.(1)
Hypoglycemia
Depletion of hepatic glycogen stores occurs because of excessive exercise and weight loss, which results in hypoglycemia. In mild cases of AN hypoglycemia rarely causes symptoms. On the contrary, severe hypoglycemia has been correlated with sudden death.(1)
Gynecologic and Reproductive Complications
In AN there is a disruption in the CNS's reproductive functions. enerally, nerve impulses trigger the secretion
of gonadotropin releasing hormone.(1) In AN there is reduced secretion of gonadotropin releasing hormone, which leads to reduced levels of luteinizing hormone and follicle stimulating hormone. As mentioned earlier, this causes amenorrhea and prevents ovulation. Usually, normal menstrual cycles start again and fertility is restored with weight gain and recovery from AN.(1)
Fertility
Despite developing amenorrhea individuals may become pregnant. In AN patients, there is a higher rate of
neonatal complications (e.g. premature birth, miscarriages, and low-birth-weight infants) and complications of
pregnancy. A diet enriched in phosphate and protein and supplementation with vitamin D and calcium is suggested.(1)
Renal and Electrolytes
AN patients may have reduced glomerular filtration rates. There have been reports of both chronic and acute renal failure.(3) Additionally, patients may have problems concentrating their urine that leads to dehydration and diuresis. With weight gain renal function normally recovers. dditionally, depletion of potassium, phosphate and magnesium may occur. Correct electrolytes and rehydrate the patient before refeeding the patient.(1)
Pulmonary
Dyspnea, weakness and wasting of respiratory muscles, decreased pulmonary capacity and reduced aerobic capacity may be observed in AN. Pneumothorax and pneumomediastinum have also been reported. (1)
Hematologic
Luekopenia, anemia, thrombocytopenia and bone marrow changes commonly
occur in AN. (1)
Gastrointestinal
AN commonly causes constipation and gastroparesis. Elevated liver function tests, acute pancreatitis and the superior mesenteric artery syndrome (rare) may also occur.(1)
Constipation
Stimulant laxatives or bulking, iber-containing laxatives may worsen constipation. 6-8 glasses of water per day and fiber in low doses may help manage onstipation. Constipation hould resolve with weight restoration. (1)
Gastroparesis
Symptoms include bloating, fullness, early satiety, heartburn, nausea, and vomiting. atients should be reassured that gastroparesis is not caused by eating and that it will resolve with weight restoration. For approximately the first two eeks of refeeding, half of the calories should come from liquid food upplements. Legume-type foods, ran products, and excessive fiber should be avoided as they may promote istension and gas. (1)
Neurologic
AN can lead to brain atrophy. Studies found that gray matter, white matter and right and left hippocampus are reduced in AN.(1,4) Moreover, hypotension and bradycardia may be caused in part by decreased levels of norepinephrine.(4) Other complications may include seizures, peripheral neuropathy and cognitive impairment.(1)
Refeeding Syndrome
"The feeding syndrome is defined as the clinical complications that occur as a result of fluid and electrolyte shifts during nutritional rehabilitation of malnourished".(5) The predominant cause and hallmark of the syndrome is hypophosphatemia. Medical complications involve multiple organ systems (e.g. cardiovascular system, gastrointestinal system). Cardiac complications are responsible for the most fatalities.(5) Introducing calories gradually versus rapidly reduces this risk of complications.(3)
Dermatologic
Trauma from burns or cuts may be present in patients secondary to
self-injurious behaviours, which are common.(1)
Symptoms of starvation include:(1)
· Xerosis (scaly, dry skin)
· Telogen effluvium (hair loss)
· Lanugo-like body hair (fine, downy, dark hair)
· Acne
· Hyperpigmentation
· Carotenoderma (yellowing)
· Seborrheic dermatitis (erythema and greasy scales)
· Perniosis (pruritic or painful erythema)
· Livedo reticularis
· Petechiae
· Pruritus
· Paronychia Acrocyanosis
· Slower wound healing
· Striae distensae (hypopigmented or erythematous linear patches)
The majority of symptoms resolve or improve with weight gain with the exception of striae distensae.(1)
Other Complications(3,6)
· Depression
· Dental complications
· Oropharyngeal complications
Structural Canges
Structural changes include reduced cardiac chamber volumes, decreased cardiac mass, atrophy of cardiac muscle, and mitral valve prolapse. These changes lead to subjective fatigue, decreased cardiac output, a decreased blood pressure response to exercise and reduced exercise capacity. The weakened heart muscle normally improves and heart size normalizes with weight gain and clinical recovery.(1)
Chest pain or palpitations may occur due to mitral valve prolapse. Additionally, HDL may increase because of weight loss and excessive exercise. There may also be insignificant elevations in LDL, however obstructive coronary disease was not revealed in autopsy studies. Furthermore, pericardial effusion is another complication that has been reported in adolescents.(1)
Functional Changes
Functional changes include hypotension, QT dispersion, diminished heart rate variability and bradycardia. In some patients QT prolongation may occur however, it is not clear whether it is a direct result of AN. (1) The ECG is often normal with the exception of bradycardia. QT dispersion may be caused by direct injury to the myocardium during starvation and is a marker for increased arrhythmic risk. Reduced heart rate variability may be associated with an increased incidence of death in AN. Furthermore, orthostatic hypotension may occur and depending on the severity may require hospitalization.(1)
Bradycardia
In a study of anorexic women, 41% were found to have bradycardia. Increased parasympathetic activity appears to be the cause of bradycardia.(1) Hospitalization is suggested by the APA guidelines if heart rate is less than 0 beats/minute. This complication normally resolves once weight is restored.(2)
Endocrine
Hypothalamus and pituitary
Starvation results in reduced secretion of gonadotropin releasing hormone, which leads to reduced levels of luteinizing hormone and follicle stimulating hormone. (1,3) Ultimately this causes amenorrhea and prevents ovulation. Moreover, there is evidence of elevated blood levels of cortisol secondary to an "increased activation of the hypothalamic-pituitary-adrenal
axis". Decreased blood levels of testosterone results in diminished production of androgens. Additionally, libido and a diminished anabolic state occur secondary to reduced testosterone. Bone formation is impeded because of decreased production of insulin-like growth factor. Furthermore, hypothermia was found in 22% of patients in a study.(1)
Osteoporosis
Osteoporosis is a potential long-term complication.(3) Amenorrhea for 6 months and a BMI of 15 kg/m2 can result in a decreased bone mineral density, which correlates with the degree of osteoporosis. The osteoporosis in postmenopausal women differs from the osteoporosis in patients with AN. For example, there are normal serum levels of vitamin D, parathyroid hormone and calcium in AN patients with osteoporosis. Resumption of menstrual function and
weight gain is the best treatment.(1)
Thyroid
Euthyroid hypothyroxinemia may develop. A normal serum level of TSH, decreased or normal serum levels of T3 and T4, and increased serum level of reverse T3 characterizes this complication. Thyroid hormone replacement is not indicated because it is not beneficial and it may be harmful.(1)
Hypoglycemia
Depletion of hepatic glycogen stores occurs because of excessive exercise and weight loss, which results in hypoglycemia. In mild cases of AN hypoglycemia rarely causes symptoms. On the contrary, severe hypoglycemia has been correlated with sudden death.(1)
Gynecologic and Reproductive Complications
In AN there is a disruption in the CNS's reproductive functions. enerally, nerve impulses trigger the secretion
of gonadotropin releasing hormone.(1) In AN there is reduced secretion of gonadotropin releasing hormone, which leads to reduced levels of luteinizing hormone and follicle stimulating hormone. As mentioned earlier, this causes amenorrhea and prevents ovulation. Usually, normal menstrual cycles start again and fertility is restored with weight gain and recovery from AN.(1)
Fertility
Despite developing amenorrhea individuals may become pregnant. In AN patients, there is a higher rate of
neonatal complications (e.g. premature birth, miscarriages, and low-birth-weight infants) and complications of
pregnancy. A diet enriched in phosphate and protein and supplementation with vitamin D and calcium is suggested.(1)
Renal and Electrolytes
AN patients may have reduced glomerular filtration rates. There have been reports of both chronic and acute renal failure.(3) Additionally, patients may have problems concentrating their urine that leads to dehydration and diuresis. With weight gain renal function normally recovers. dditionally, depletion of potassium, phosphate and magnesium may occur. Correct electrolytes and rehydrate the patient before refeeding the patient.(1)
Pulmonary
Dyspnea, weakness and wasting of respiratory muscles, decreased pulmonary capacity and reduced aerobic capacity may be observed in AN. Pneumothorax and pneumomediastinum have also been reported. (1)
Hematologic
Luekopenia, anemia, thrombocytopenia and bone marrow changes commonly
occur in AN. (1)
Gastrointestinal
AN commonly causes constipation and gastroparesis. Elevated liver function tests, acute pancreatitis and the superior mesenteric artery syndrome (rare) may also occur.(1)
Constipation
Stimulant laxatives or bulking, iber-containing laxatives may worsen constipation. 6-8 glasses of water per day and fiber in low doses may help manage onstipation. Constipation hould resolve with weight restoration. (1)
Gastroparesis
Symptoms include bloating, fullness, early satiety, heartburn, nausea, and vomiting. atients should be reassured that gastroparesis is not caused by eating and that it will resolve with weight restoration. For approximately the first two eeks of refeeding, half of the calories should come from liquid food upplements. Legume-type foods, ran products, and excessive fiber should be avoided as they may promote istension and gas. (1)
Neurologic
AN can lead to brain atrophy. Studies found that gray matter, white matter and right and left hippocampus are reduced in AN.(1,4) Moreover, hypotension and bradycardia may be caused in part by decreased levels of norepinephrine.(4) Other complications may include seizures, peripheral neuropathy and cognitive impairment.(1)
Refeeding Syndrome
"The feeding syndrome is defined as the clinical complications that occur as a result of fluid and electrolyte shifts during nutritional rehabilitation of malnourished".(5) The predominant cause and hallmark of the syndrome is hypophosphatemia. Medical complications involve multiple organ systems (e.g. cardiovascular system, gastrointestinal system). Cardiac complications are responsible for the most fatalities.(5) Introducing calories gradually versus rapidly reduces this risk of complications.(3)
Dermatologic
Trauma from burns or cuts may be present in patients secondary to
self-injurious behaviours, which are common.(1)
Symptoms of starvation include:(1)
· Xerosis (scaly, dry skin)
· Telogen effluvium (hair loss)
· Lanugo-like body hair (fine, downy, dark hair)
· Acne
· Hyperpigmentation
· Carotenoderma (yellowing)
· Seborrheic dermatitis (erythema and greasy scales)
· Perniosis (pruritic or painful erythema)
· Livedo reticularis
· Petechiae
· Pruritus
· Paronychia Acrocyanosis
· Slower wound healing
· Striae distensae (hypopigmented or erythematous linear patches)
The majority of symptoms resolve or improve with weight gain with the exception of striae distensae.(1)
Other Complications(3,6)
· Depression
· Dental complications
· Oropharyngeal complications
Table 5. "Physical and Laboratory Assessment of Eating Disorders"(3)
Reference
1. Mehler P. Anorexia nervosa in adults and adolescents: Medical complications and their management. UpToDate. http://www.uptodate.com/contents/anorexia-nervosa-in-adults-and-adolescents-medical-complications-and-their-management. Updated May 23, 2013. Accessed June 1, 2013.
2. Treatment of patients with eating disorders,third edition. American Psychiatric Association. American Psychiatric Association. Am J Psychiatry. 2006;163(7 Suppl):4-54.
3 . Talbert RL, DiPiro JT, Matzke GR, Posey LM, Wells BG, Yee GC. Chapter 64. Multiple Sclerosis. In: Pharmacotherapy: A Pathophysiologic Approach. 8th ed. New York: McGraw-Hill; 2011. http://www.accesspharmacy.com/content.aspx?aID=7984977. Accessed June 1, 2013.
4. Forman SF. Eating disorders: Epidemiology, pathogenesis, clinical features, and course of illness. UpToDate. http://www.uptodate.com/contents/eating-disorders-epidemiology-pathogenesis-clinical-features-and-course-of-illness. Updated September 25, 2012. Accessed June 1, 2013.
5. Mehler P. Anorexia nervosa in adults and adolescents: The refeeding syndrome. UpToDate. http://www.uptodate.com/contents/anorexia-nervosa-in-adults-and-adolescents-the-refeeding-syndrome. Updated May 15, 2013. Accessed June 1, 2013.
6. Anorexia Nervosa. DynaMed. http://web.ebscohost.com/dynamed/detail?vid=3&sid=b9c41bae-db1d-4f87-bca4-5bfac549946f%40sessionmgr112&hid=123&bdata=JnNpdGU9ZHluYW1lZC1saXZlJnNjb3BlPXNpdGU%3d#db=dme&AN=114614. Updated February 20, 2013. Accessed June 1, 2013.
Image
1. Anorexia nervosa factsheet. womenshealth.gov. http://womenshealth.gov/publications/our-publications/fact-sheet/anorexia-nervosa.cfm. Updated June 15, 2009. Accessed June 1, 2013.
1. Mehler P. Anorexia nervosa in adults and adolescents: Medical complications and their management. UpToDate. http://www.uptodate.com/contents/anorexia-nervosa-in-adults-and-adolescents-medical-complications-and-their-management. Updated May 23, 2013. Accessed June 1, 2013.
2. Treatment of patients with eating disorders,third edition. American Psychiatric Association. American Psychiatric Association. Am J Psychiatry. 2006;163(7 Suppl):4-54.
3 . Talbert RL, DiPiro JT, Matzke GR, Posey LM, Wells BG, Yee GC. Chapter 64. Multiple Sclerosis. In: Pharmacotherapy: A Pathophysiologic Approach. 8th ed. New York: McGraw-Hill; 2011. http://www.accesspharmacy.com/content.aspx?aID=7984977. Accessed June 1, 2013.
4. Forman SF. Eating disorders: Epidemiology, pathogenesis, clinical features, and course of illness. UpToDate. http://www.uptodate.com/contents/eating-disorders-epidemiology-pathogenesis-clinical-features-and-course-of-illness. Updated September 25, 2012. Accessed June 1, 2013.
5. Mehler P. Anorexia nervosa in adults and adolescents: The refeeding syndrome. UpToDate. http://www.uptodate.com/contents/anorexia-nervosa-in-adults-and-adolescents-the-refeeding-syndrome. Updated May 15, 2013. Accessed June 1, 2013.
6. Anorexia Nervosa. DynaMed. http://web.ebscohost.com/dynamed/detail?vid=3&sid=b9c41bae-db1d-4f87-bca4-5bfac549946f%40sessionmgr112&hid=123&bdata=JnNpdGU9ZHluYW1lZC1saXZlJnNjb3BlPXNpdGU%3d#db=dme&AN=114614. Updated February 20, 2013. Accessed June 1, 2013.
Image
1. Anorexia nervosa factsheet. womenshealth.gov. http://womenshealth.gov/publications/our-publications/fact-sheet/anorexia-nervosa.cfm. Updated June 15, 2009. Accessed June 1, 2013.
